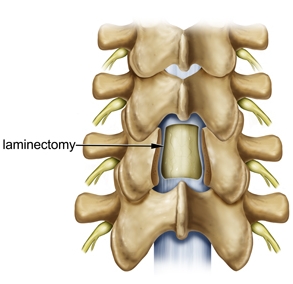
Laminectomy is a spine surgery that involves removing bone to relieve excess pressure on the spinal nerve(s). A lumbar laminectomy is often performed to relieve the symptoms of spinal stenosis and the narrowing of the spinal canal and may be done using minimally invasive surgery. The term laminectomy is derived from the Latin words lamina (thin plate, sheet, or layer), and -ectomy (removal). A laminectomy removes or “trims” the lamina (roof) of the vertebrae to create space for the nerves leaving the spine.
Traditional, open spine surgery involves cutting or stripping the muscles from the spine. But today, a lumbar laminectomy may be performed using minimally invasive spine surgery, a treatment that involves small incisions and muscle dilation, allowing the surgeon to gently separate the muscles surrounding the spine rather than cutting them.
Why do I need a lumbar laminectomy?
Spinal stenosis is a condition caused by a gradual narrowing of the spinal canal. This narrowing happens as a result of the degeneration of both the facet joints and the intervertebral discs. In this condition, bone spurs, called osteophytes, which develop because of the excessive load on the intervertebral disc, grow into the spinal canal. The facet joints also enlarge as they become arthritic, which contributes to a decrease in the space available for the nerve roots. The ligaments of the spinal column, especially the ligamentum flavum, become stiff, less flexible, and thicker with age, which also contributes to spinal stenosis. These processes narrow the spinal canal and may begin to impinge and put pressure on the nerve roots and spinal cord, creating the symptoms of spinal stenosis.
How is the procedure performed?
The operation is performed with the patient on his or her stomach.
Accessing the Spine
First, the surgeon makes a small incision. Through this incision, the muscle will be gently and gradually dilated, or separated, and a tubular retractor will be inserted to create a portal through which the surgeon may perform minimally invasive surgery.
Laminectomy
Part of the lamina is cut away to uncover the ligamentum flavum—a ligament that supports the spinal column. Next, an opening is cut in the ligamentum flavum, through which the spinal canal is accessed. The compressed nerve is now visible, as is the cauda equina (the bundle of nerve fibers at the end of the spinal cord) to which it is attached. This procedure allows the surgeon to determine the source of nerve compression.
Implant Placement
Sometimes it is necessary for the surgeon to also stabilize the spine by fusing the vertebrae, a procedure called spinal fusion. Spinal fusion involves placing bone graft material between adjacent vertebrae to promote bone growth that joins the two structures. Instrumentation such as plates, cages, screws, and rods also may be used to create an “internal cast” to stabilize the spine while fusion takes place.
Your surgeon will then close the incision, which typically leaves behind only a small scar if a minimally invasive procedure is performed.
After Surgery
This minimally invasive procedure typically allows many patients to be discharged on the same day of surgery; however, some patients may require a longer hospital stay. Many patients will notice immediate improvement of some or all of their symptoms; other symptoms may improve more gradually.
A positive attitude, reasonable expectations, and compliance with your doctor’s post-surgery instructions all may contribute to a satisfactory outcome. Many patients are able to return to their regular activities within several weeks.